
What to do if your child knocks out or fractures a tooth. Evidence-based pediatric dental trauma care and prevention in Los Angeles.
Knowledge Welcomes Confidence and Empowerment
As a pediatric dentist, I have received many calls from frantic parents whose children have bumped their teeth at home, at school, or while playing sport. My heart goes out to the parents of toddlers who turn their heads for a split second only to hear a loud thud followed by explosive cries. I think of parents receiving a call from school informing them that their child has had an accident on the playground. And of course, the young athletes in the middle of a game who get hit by balls, elbows, or even feet.
The purpose of writing this is primarily to reassure parents that they are doing their best. As much as we love and protect our children, they will experience their own journeys. Our role is to remain informed, supportive, and calm and to trust in modern, evidence-based dental care when it is needed most.
My hope is that this blog serves as a quick, practical reference for what to do during a dental trauma emergency: how to respond, how to comfort your child, and how to understand the appropriate timeframe for management based on decades of scientific research that have shaped today’s state-of-the-art pediatric dentistry.
Most importantly, I hope it offers reassurance in that our children are resilient, and with, gentle and attentive care, they can return to oral health and well-being.
How To Manage Dental Injuries
In moments of trauma, parents are suddenly confronted with uncertainty. They are not only trying to comfort their child but are also searching for answers. The good news is that there are a few key actions that significantly improve outcomes. These steps are simple, easy to remember, and can be implemented immediately.
Emergency calls to our office at Smiles Pediatric Dentistry & Orthodontics are always given priority. These calls are essential in guiding parents in real time. Immediate communication allows us to assess the situation, determine the urgency, and provide clear next steps.
Teledentistry has become an especially valuable tool in these circumstances. Virtual assessment allows us to evaluate kids quickly wherever they are, guide first-line management, and coordinate appropriate follow-up care. Just as importantly, it offers reassurance at a time of uncertainty. Parents and children benefit from knowing they are supported with presence, knowledge, and compassion.
Many dental trauma incidents can be managed outside of the emergency room. When a call comes in, one of the first decisions we review is whether medical evaluation is necessary. If we determine that the injury was purely dental in nature, we efficiently shift gear into the prompt management of the trauma to help ensure the most positive outcome.
If there is concern for head injury, loss of consciousness, nausea, dizziness, or significant soft tissue trauma, medical care must come first because every child’s overall well-being always takes priority. When children do present to the emergency room, medical triage appropriately takes priority. Soft tissue injuries may require suturing. Imaging and neurological evaluation take time. These essential steps can inadvertently delay time-sensitive dental intervention. However, early dental triage, even if coordinated alongside medical care, is both possible and beneficial.
The Evidence Behind Modern Dental Trauma Care
All of us in the pediatric dental profession hold a special place in our hearts for the father of modern dental traumatology, Dr. Jens Andreasen. His evidence-based work, spanning more than six decades, has not only stood the test of time but continues to serve as the foundation for how we diagnose, triage, and manage dental trauma today.
As a child who personally experienced dental trauma, Dr. Andreasen new firsthand what a child goes through when they deal with a dental injury. He dedicated his career to understanding what happens to injured teeth, and more importantly, how to save them. His research taught us something powerful: when teeth are handled properly and treated quickly, they can often be preserved. He helped establish the timeframes that matter, the safest ways to stabilize injured teeth, and why careful follow-up is essential to ensure long-term healing. Much of what we know today about managing knocked-out, displaced, or fractured teeth comes directly from his life’s work.
The International Association of Dental Traumatology (IADT) guidelines are grounded in this body of evidence and have been adopted by the American Academy of Pediatric Dentistry (AAPD). When these principles are followed, outcomes improve significantly.
Primary vs Permanent Tooth Injuries: Why Management Differs
Another important distinction we make during every trauma call is the age of the child and whether the injured tooth is primary (baby) or permanent. This information is important because it not only helps guide parents and children through the experience in an age-appropriate way, but it also directly influences how the injury is managed. Treatment decisions differ significantly depending on whether the affected tooth is primary or permanent.
Clinical management must consider anatomy, stage of root development, and long-term prognosis. It is important to understand that certain interventions that are necessary for permanent teeth may not be appropriate for primary teeth. Protecting the developing permanent tooth is always a priority when managing trauma to primary teeth.
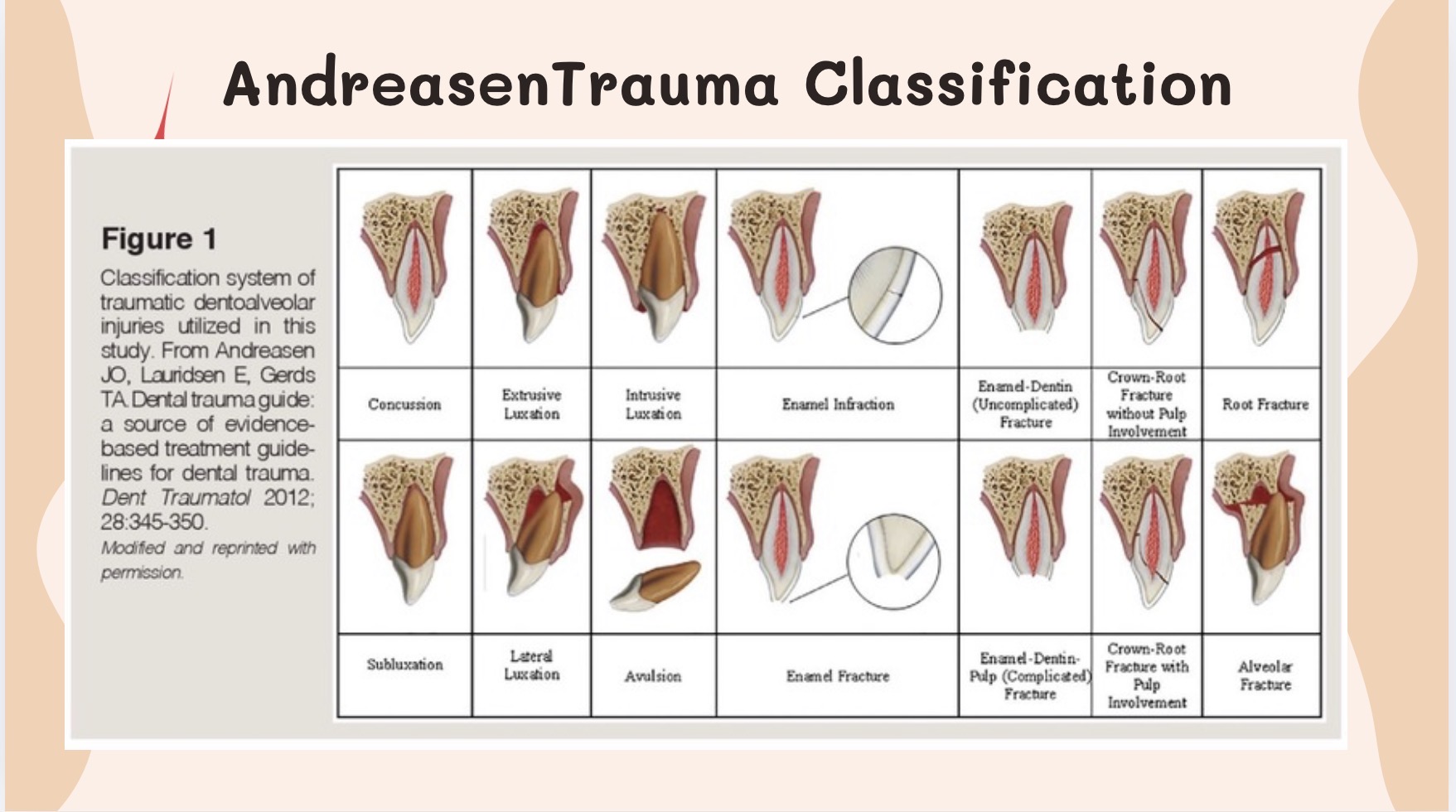
Types of Dental Injuries:
Dental trauma can present in diverse ways, depending on how the tooth is injured:
- Enamel fractures – minimal crown fractures involving only the outer white layer of the tooth.
- Enamel-dentin fractures – moderate crown fractures that extend deeper into the tooth structure but do not expose the nerve.
- Complicated crown fractures – fractures that involve pulp (nerve) exposure and often require more urgent intervention.
- Crown-root fractures – fractures that extend below the gumline, often at an angle, and may affect both the visible portion of the tooth and the root.
- Luxation injuries – injuries in which a tooth is displaced from its normal position in varying degrees or directions. These include concussion (tender but not loose), subluxation (loose but not displaced), extrusion (partially pulled out), lateral luxation (pushed sideways), and intrusion (pushed deeper into the socket).
- Avulsion – a tooth that has been completely knocked out of the mouth.
How Are Dental Injuries Managed?
Accurate diagnosis requires careful clinical examination and dental imaging (x-rays) assessment. Once all the information has been gathered, a thoughtful, evidence-based, and age-appropriate plan is followed.
Treatment decisions are guided by:
-The age of the child
-Stage of root development (a brand-new tooth vs one that has been in the mouth for years)
-Presence or absence of pulp (nerve) exposure
-Degree of mobility or displacement
-Dental imaging findings
What To Expect for Management of Dental Injuries
| Injury Type | Primary Tooth Management | Permanent Tooth Management |
| Crown fracture (chipped tooth) | Sharp edges are smoothed or the tooth is restored as needed. Pulp (nerve) vitality is monitored over time. | If the fragment is available, it may be reattached. Otherwise restored with bonding. Pulp (nerve) vitality is monitored. |
| Complicated crown fracture (pulp exposure) | Pulp therapy may be indicated depending on stage of development. Extraction may be considered if prognosis is poor. | Vital pulp therapy preferred in immature teeth. Root canal therapy may be indicated in mature teeth. |
| Crown-root fracture | Tooth assessed for restorability. Extraction may be required depending on fracture extent. | Requires stabilization and possible root canal or periodontal management depending on fracture depth. |
| Luxation injury (displaced tooth) | Often managed conservatively. Monitored closely for healing and impact on permanent successor. | Repositioning often indicated. Flexible splinting per IADT guidelines. Long-term pulp (nerve) monitoring is essential. |
| Avulsion (knocked-out tooth) | Avulsed primary teeth are not replanted. Space management or restorative options may be discussed. | Time-sensitive emergency. Tooth should be replanted immediately when possible. Stabilization required. Root canal therapy often necessary. |
What Parents Should Do Immediately After Dental Trauma
For any dental injury, try to stay as calm as you can. Comfort and reassure your child, then contact your pediatric dentist as soon as possible. Even injuries that appear minor should be evaluated to ensure proper healing and to prevent long-term complications.
Quick Guide Steps:
1. Gently clean your child’s lips and gums with a clean gauze or cloth.
2. Locate any fractured fragment and store it in water or saline.
3. If a permanent tooth is knocked out, handle it only by the crown, never the root. Try to gently reposition it into the socket and seek immediate care.
- If you are unable to reposition the tooth, placing it in a “save-a-tooth” kit https://www.saveatooth.com/ or in milk is the next best option.
- If a primary tooth is knocked out, keep it for dental evaluation but do not attempt to replant it. Primary teeth are not replanted to avoid damage to the underlying developing permanent tooth.
7. Contact your dentist promptly for evaluation.
What Parents Should Do: Immediate first steps you can take before professional evaluation
| Injury Type | What Parents Should Do – Primary (Baby) Tooth | What Parents Should Do – Permanent Tooth |
| Crown fracture (chipped tooth) | Look for the fragment to bring to your dentist. Store it in water or saline. | Look for the fragment. Store it in water or saline (not milk). |
| Complicated crown fracture (pulp exposure) | Avoid biting into foods. Avoid hot or cold foods and touching the injured area. If a fragment is present, store it in water or saline. | Avoid biting into foods. Save the fragment in water or saline if available. |
| Crown-root fracture | Do not manipulate the tooth. Keep your child comfortable. If a fragment is present, store it in water or saline. | Do not manipulate the tooth. Avoid biting on it. If a fragment is present, store it in water or saline. |
| Luxation injury (displaced tooth) | Do not attempt to reposition at home. Offer soft foods only. | Do not force the tooth back unless instructed. Avoid biting on it. |
| Avulsion (knocked-out tooth) | Do not replant. Apply gentle pressure with gauze if bleeding. Bring the tooth with you for evaluation. | Pick up the tooth by the crown only. If dirty, gently rinse with milk or saline (do not scrub). Replant immediately if possible or store in milk. Seek care within 60 minutes. |
The Importance of Follow-Up
Dental trauma management extends beyond the initial treatment. Follow-up evaluations are needed to assess the vitality of the tooth and the continued root integrity. Standard intervals often include assessments at 6–8 weeks, 6 months, and 1 year, with extended monitoring when indicated.

Prevention: The Best Treatment Is Protection
While modern dentistry allows us to manage trauma conservatively and effectively, prevention remains the most powerful intervention.
Recent collaboration between the International Association of Dental Traumatology (IADT) and the American Society of Dentistry (ASD) reflects a shared emphasis on prevention as an integral component of trauma care. This alignment highlights the importance of evidence-based protective strategies for children and adolescents engaged in athletics. With more kids involved in athletics, especially with major athletic events approaching in Los Angeles, protective measures must evolve alongside clinical innovation.

As an active member of the ASD, I remain very focused on streamlined fabrication of sports mouthguards, exploring advancements in digital workflows, material science, and precision 3D fabrication. Custom 3D printed sports guards provide superior fit, comfort, and protection compared to stock alternatives. Studies have proven that when properly fabricated and worn consistently, they significantly reduce the incidence and severity of dental injuries.
When Replacement Is Needed: Innovative Pediatric Solutions:
While prevention remains the most powerful strategy, some injuries result in tooth loss or structural damage that requires restorative intervention.
For very young patients, esthetic options for lost primary incisors were historically limited. In many cases, families were told to simply wait for the permanent teeth to erupt. Today, digital dentistry allows us to offer thoughtful alternatives.
In our practice, we utilize digital workflows to fabricate conservative, esthetic solutions for young patients — including PrintiSmile™, a custom-designed 3D printed pediatric anterior restoration.
Unlike traditional removable appliances or aggressive preparations, PrintiSmile™ allows for:
- Precise digital design
- Minimal intervention
- Age-appropriate esthetics
- Efficient chairside delivery
For children navigating early childhood social development, restoring the appearance of a front tooth can support confidence, speech development, and overall well-being. Digital pediatric dentistry allows us to restore both biology and self-confidence.

Clinical Case: Uncomplicated Crown Fracture in a Teen Athlete
When life presents unexpected challenges, thoughtful care can turn a stressful moment into a positive outcome.
A teen athlete presented with an uncomplicated crown fracture of a maxillary central incisor following trauma. Because he was undergoing Invisalign therapy at the time of injury, his aligner tray was utilized as a precision positioning guide during fragment reattachment.
This allowed accurate adaptation of the rebonded fragment while preserving natural anatomy. The result achieved excellent esthetics with minimal intervention, demonstrating the value of prompt evaluation and conservative treatment planning.
👉 If your child has experienced a chipped, displaced, or knocked-out tooth, contact Smiles Pediatric Dentistry & Orthodontics for expert pediatric dental trauma care. Our team provides treatment to protect your child’s smile and help prevent long-term complications.
Contact us to schedule an appointment or book a consultation through our website.
Frequently Asked Questions About Pediatric Dental Trauma
What should I do if my child knocks out a permanent tooth?
Pick up the tooth by the crown only. Reinsert the tooth immediately into its socket, if possible, or store in milk and seek care within 60 minutes.
Should I replant a baby tooth that was knocked out?
No. Primary teeth should not be replanted due to risk to the developing permanent tooth.
Can a chipped tooth fragment be rebonded?
Yes. If preserved properly in water or saline, many permanent tooth fragments can be successfully rebonded.
How long can a tooth stay out of the mouth?
Prognosis declines significantly after 60 minutes of dry time. Immediate action improves survival.
Does my child need a mouthguard for sports?
Yes. Custom sports mouthguards significantly reduce the incidence and severity of dental injuries.
References
Andreasen JO, Andreasen FM, Andersson L. Textbook and Color Atlas of Traumatic Injuries to the Teeth.
International Association of Dental Traumatology (IADT) Guidelines for the Management of Traumatic Dental Injuries.
American Society of Dentistry (ASD) Collaborative Guidance on Trauma Prevention and Protective Fabrication.